18
In a newly published single-patient report titled “Paraspinal Skip Lesion Encountered During the Resection of a Sacral Chordoma: A Case Report,” surgeons describe finding a discontinuous paraspinal tumor focus separate from the primary sacral mass during surgery. While a solitary case cannot establish prevalence, the observation highlights a wider systems issue for oncology programs and payers: sacral chordoma may present with complex, multifocal patterns of disease that strain imaging, surgical planning, and post‑operative control strategies across hospitals and insurance networks.
What a paraspinal “skip lesion” signals in sacral chordoma
- Definition in practice: a noncontiguous tumor deposit located away from the primary sacral chordoma, detected intraoperatively or on imaging, effectively behaving as a separate geometric focus of disease.
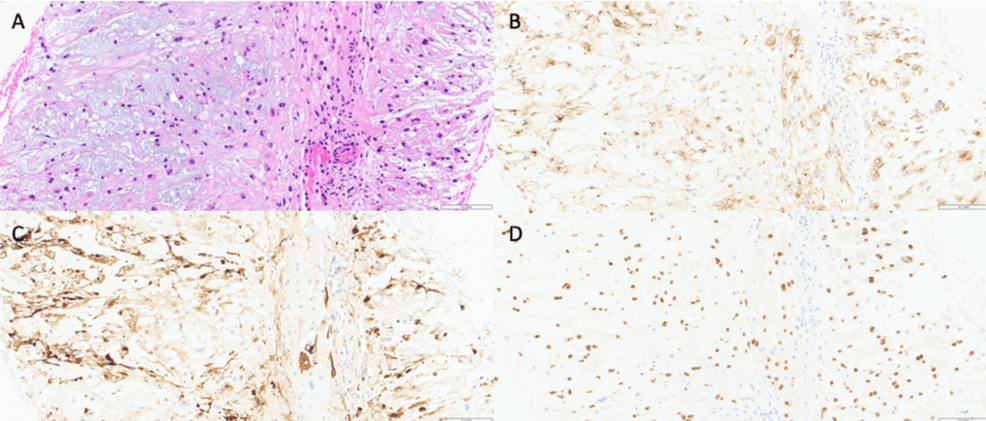
- Implication for surgical policy and planning: beyond standard margin control, teams must anticipate microscopic or macroscopic foci that can complicate resection margins and adjuvant targeting. Evidence of chordoma “micro‑skip” spread in surrounding tissues has been described histologically, underscoring the need for meticulous margin strategy, preauthorized access to advanced imaging, and long‑term surveillance planning.
- Population context: chordoma is rare in the United States-about 0.088 cases per 100,000 persons annually-with sacral tumors comprising roughly one‑third of cases and a male predominance. For hospital leaders, this low volume often means a small number of highly complex patients whose care pathways are disproportionately affected by referral patterns and benefit design.
Imaging and operative planning: gaps the case brings into focus
- Preoperative mapping: cross‑sectional imaging of the primary site and adjacent compartments is the baseline in chordoma work‑ups conducted by multidisciplinary teams. Consensus frameworks emphasize comprehensive anatomic delineation to guide en bloc resection and adjuvant radiotherapy planning, but the appearance of an unexpected skip lesion highlights how easily disease can extend beyond conventional fields if imaging protocols are inconsistently applied.
- Target definition after resection: recurrent sacral chordoma often emerges in multifocal patterns across nearby sacral segments and soft tissues, challenging narrow target volumes and standard expansions. Recent analyses propose larger, individualized postoperative target concepts when feasible, putting pressure on radiation services to reconcile aggressive targeting with dose constraints to bowel, nerves, and pelvic organs.
- Intraoperative surprises: a paraspinal skip focus discovered at surgery can force on‑the‑spot changes to planned margins, reconstruction, and adjuvant strategies, with downstream effects on wound risk, nerve preservation, and rehabilitation resources noted in sacral series. For operating hospitals, this translates into contingency planning for additional operative time, implants, blood products, and specialized post‑acute care.
System and policy dimensions: where patients are treated matters
- Multidisciplinary capacity: guideline frameworks call for care in centers with expertise in chordoma, integrating complex spine, colorectal, plastic reconstruction, radiation oncology, pathology, and rehabilitation services. This infrastructure is essential when intraoperative findings alter the surgical plan, and it increasingly informs regional referral agreements and network adequacy standards negotiated between payers and large systems.
- Advanced radiation access: proton therapy is frequently used for chordoma when high-dose conformality is required near critical nerves and bowel. In the United States, Medicare coverage is shaped by local and national determinations under the Proton Beam Therapy Local Coverage Determination, but real‑world utilization still depends on regional availability, prior authorization, and whether patients can travel to designated centers within the time windows oncologists recommend.
- Heavy‑ion readiness: carbon‑ion therapy-used internationally for radioresistant tumors-is moving toward limited U.S. availability. Mayo Clinic’s Jacksonville program, now housed in a new facility, projects proton treatments in 2027 and carbon ions in 2028, potentially expanding options for anatomically constrained chordomas. For regulators and payers, these timelines foreshadow future debates over indication‑specific coverage, capital investment, and cross‑state referral flows.
Data at a glance
| Measure | Most relevant figures/insights |
|---|---|
| Incidence (U.S.) | ~0.088 per 100,000 persons per year; sacral ~34% of cases; male predominance (IRR ~1.5). For planners, this means small absolute numbers but high complexity concentrated in tertiary centers. |
| Sacral chordoma survival | 5‑year relative survival ~60% in SEER cohort (1974-2011), with outcomes closely linked to adequacy of initial local control and access to high‑dose radiation. |
| Recurrence behavior after surgery | Recurrent disease frequently multifocal within sacral and adjacent soft‑tissue regions, complicating target delineation and creating a recurring need for advanced imaging, multidisciplinary review, and, in some cases, repeat high‑cost interventions. |
| Operative principle | Margin‑negative en bloc resection is linked to better local control when achievable by anatomy and function, but demands specialized teams, robust perioperative infrastructure, and coverage structures that support referral to centers of excellence. |
| Coverage & access | Proton therapy is often covered for chordoma under Medicare and many commercial policies; however, facility availability, prior authorization, and patient travel constraints remain rate‑limiting factors in timely delivery of recommended care. |
Operational implications for hospitals and payers
- Perioperative resources: sacral resections may require staged plastic closure, ostomy capabilities, and lumbopelvic stabilization, particularly when intraoperative findings extend resection beyond plan. Resource forecasts should include wound care, intensive nursing, and inpatient rehabilitation capacity, as well as out‑of‑network and transfer protocols for hospitals that lack these capabilities.
- Imaging protocols: the case reinforces a conservative approach to mapping possible noncontiguous disease pre‑ and post‑operatively, coupled with durable surveillance programs led by experienced radiology and spine oncology teams. Standardizing these protocols-often through tumor boards and enterprise imaging policies-can reduce variation in how rare tumors are staged and followed.
- Payment policy: proton therapy access remains uneven; health plans’ local determinations list chordoma among indications, but center proximity and authorization timelines can delay care. As carbon‑ion programs enter the U.S. ecosystem, they are likely to prompt new coverage frameworks, including how plans define “medically necessary” use and when they will support cross‑regional referrals.
Equity and rare‑disease logistics
- Demographics and delays: incidence rises with age, and men have higher risk-features that intersect with mobility, caregiver availability, and coverage characteristics in older adults. For public payers, that raises questions about transportation benefits, lodging support, and how to avoid treatment delays rooted in nonclinical barriers.
- Geography of technology: proton centers cluster regionally, and the first U.S. carbon‑ion site is planned for Florida-travel and housing support will remain material barriers unless addressed explicitly in benefit design or philanthropic programs. State regulators and hospital boards will face decisions about whether to invest in satellite services, tele‑tumor boards, or shared‑care models to keep patients from being stranded far from home.
Policy and practice anchors (limited selection)
- Clinical management frameworks are detailed in the peer‑reviewed NCCN Bone Cancer guidelines, which emphasize multidisciplinary evaluation, cross‑sectional imaging, and margin‑oriented surgery for chordoma when feasible. These guidelines, developed through a consensus process, now function effectively as a soft regulatory standard against which hospital pathways and payer medical policies are often benchmarked.
- For coverage, Medicare contractors list chordoma among indications for proton beam therapy in the Proton Beam Therapy Local Coverage Determination, aligning federal reimbursement policy with the requirement for high‑dose conformal radiation in anatomically constrained tumors while leaving room for contractors to refine utilization criteria over time.
The takeaway for health systems
- Single cases do not change standards, but a surgically discovered paraspinal skip lesion in sacral chordoma is a sharp reminder that disease geometry can outpace routine plans. Health systems that standardize multidisciplinary review, invest in advanced imaging and radiation capabilities, and streamline coverage and referral pathways-particularly for rare, high‑stakes tumors-are best positioned to prevent avoidable re‑operations, missed disease, and treatment delays that emerge at the intersection of biology and policy.