Study signals potential for simple blood-count ratios to flag PPROM risk
Preterm premature rupture of membranes (PPROM) remains a major driver of preterm birth and neonatal complications, accounting for a substantial share of births before 37 weeks in the United States and globally. New peer‑reviewed research identifies routine complete blood count-derived ratios as potential early biomarkers, raising questions about whether low‑cost laboratory signals could help stratify risk before complications escalate or require higher‑acuity care. In a single‑center cohort published in Cureus, researchers compared neutrophil‑to‑lymphocyte ratio (NLR) and platelet‑to‑lymphocyte ratio (PLR) among pregnant patients with PPROM and those delivering at term, while excluding people with active infection to focus on inflammation‑related patterns unrelated to overt sepsis. The authors report: “NLR was significantly higher in the PPROM group than in the control group (p=0.001).”
- Clinical focus: identifying inflammation‑linked hematologic patterns associated with membrane rupture before 37 weeks
- Why it matters: inexpensive, widely available tests could enhance risk flagging in settings without access to specialized biomarker assays or advanced perinatal imaging
What the researchers measured and what they found
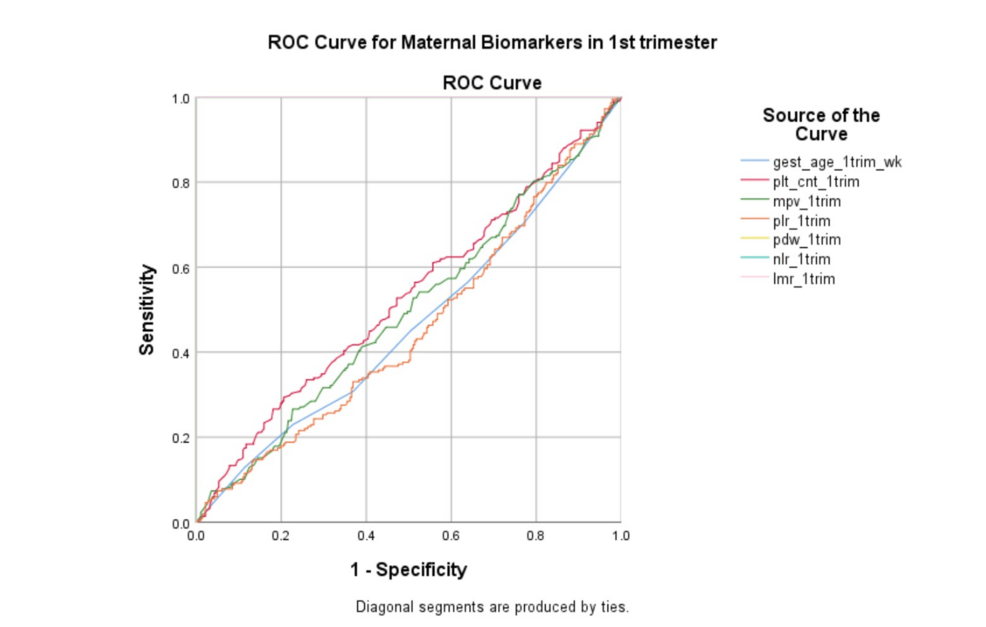
The cohort drew on pregnancies between 22-34 weeks with PPROM and term controls from a high‑volume tertiary center. Key measures included absolute neutrophil, lymphocyte, and platelet counts; derived NLR and PLR; and gestational‑age subgroup analyses. The study team emphasized the potential for a simple index to differentiate higher‑risk presentations: “NLR cutoff of 6.73 was obtained for PPROM occurrence.” While PLR was elevated in a subset, the authors noted, “In our study, although PLR was not statistically significant between the PPROM and control groups (p>0.05).”
| Measure | Finding | Study detail |
|---|---|---|
| Study population | PPROM n=67; controls n=91 | Single center; all participants with normal C‑reactive protein at enrollment |
| NLR (overall pattern) | Higher in PPROM vs control | Group means across PPROM subgroups around 6.0 vs 3.8 in controls |
| NLR diagnostic performance | Cutoff 6.73 | Reported area under the curve 0.671 (95% CI 0.587-0.755) |
| PLR | Not significant overall | Significant only at 25-30 weeks subgroup (p=0.03) |
| Design caveat | Single-center cohort | Authors highlight the need for gestational‑age-specific thresholds and larger validation |
These signals underscore the appeal of complete blood count-derived ratios: rapid turnaround, negligible incremental cost, and integration with existing antenatal workflows that already rely on routine laboratory panels. Yet modest discrimination (AUC 0.671) and gestational‑age effects mean ratios are not ready for stand‑alone screening or for use as a definitive diagnostic tool.
Full paper: Cureus study on hematologic ratios and PPROM risk (open access).
How this fits within current obstetric practice
In current U.S. care, evaluation and management of PPROM are anchored in clinical assessment, gestational age, and shared decision‑making, not blood‑based screening. Professional guidance emphasizes individualized counseling, timed use of antibiotics, antenatal corticosteroids, and context‑specific obstetric interventions, particularly around thresholds for delivery versus expectant management. Those frameworks provide an interpretive backdrop for any new biomarker‑based tool, which would need to complement-not replace-established pathways shaped by national practice standards and payer policies.
At present, hematologic ratios such as NLR and PLR are best viewed as investigational markers that may refine existing risk conversations rather than drive them. For example, they could be incorporated into research protocols that combine laboratory values with cervical length or prior preterm birth history to test whether multi‑parameter models meaningfully change counseling or timing of transfer to higher‑level centers.
- Use case today: potential adjunct for risk stratification in research settings or tightly governed quality‑improvement projects
- Clinical guardrails: ratios should not drive management decisions-such as admission, transfer, or delivery timing-without corroborating clinical evidence
- Regulatory and guideline reality: broad adoption would require multicenter validation, analytical standardization across laboratories, and demonstration of clinical utility before professional societies or major payers considered formal endorsement
Any future integration of NLR‑based tools would need to align with the oversight expectations of agencies such as the U.S. Food and Drug Administration, which regulates in vitro diagnostic devices and clinical decision‑support software that may influence patient management.
Public‑health considerations and system impact
Because PPROM contributes materially to prematurity, neonatal intensive‑care admissions, and long‑term developmental risk, even small gains in early identification can have outsized system effects. The policy question is whether a marker like NLR can help health systems deploy scarce resources-specialist consultations, transport to higher‑acuity centers, and intensive monitoring-more efficiently and equitably.
- Equity and access
- Routine CBCs are ubiquitous, lowering barriers for safety‑net systems and rural clinics that may lack access to advanced biomarker assays or 24/7 imaging
- Low‑cost markers may help target enhanced surveillance where specialist access is limited, potentially informing regional perinatal transfer protocols
- Implementation risks
- False positives could prompt unnecessary transfers, admissions, or early deliveries if ratios are applied outside validated thresholds or without standardized interpretation
- Gestational‑age variability argues for local calibration, clear reporting standards, and explicit governance over how thresholds are used in triage algorithms
- Workforce and workflow
- Automated flagging in electronic health records could support nurse‑led triage and maternal‑fetal medicine consults, but would need oversight to avoid alarm fatigue
- Any deployment would require protocols for confirmatory assessment, documentation, and escalation pathways across on‑call teams and referral networks
- Economic lens
- Minimal marginal cost per test contrasts with high direct and downstream costs of late recognition of PPROM‑related complications, including prolonged neonatal intensive‑care stays
- Payers and public programs would likely require outcome‑based evidence-such as reduced severe neonatal morbidity or avoidable transfers-before endorsing use in coverage or value‑based purchasing policies
Interpreting the signal: strengths, limits, and next steps
For hospital leaders, policymakers, and clinicians alike, the question is not whether NLR is statistically different in PPROM but whether that difference can be translated into reliable, actionable decisions that improve outcomes without unintended harms.
- Strengths
- Uses data available in virtually all obstetric settings, from tertiary centers to smaller community hospitals
- Signals persist even when overt infection is excluded, suggesting an association with underlying inflammatory processes rather than only acute sepsis
- Limits
- Modest discriminatory power; not a diagnostic test and unlikely to serve as a solitary screening tool
- Ratio values can be influenced by comorbidities, medications, and the physiological changes of pregnancy, complicating universal cutoffs
- Single‑center design; external validity across different populations, care models, and laboratory platforms remains to be tested
- Research and governance needs
- Prospective, multicenter cohorts with prespecified, gestational‑age-specific cutoffs and clear analytic standards
- Integration with clinical features (e.g., cervical length, prior preterm birth, maternal comorbidities) to evaluate multi‑parameter models that reflect real‑world decision‑making
- Health‑system studies to quantify downstream effects on referrals, admissions, timing of delivery, and maternal‑neonatal outcomes, including cost‑effectiveness
- Policy‑oriented work to define when an NLR‑based tool would constitute a regulated diagnostic or decision‑support product, and what evidence bar it must meet
The authors’ bottom line remains concise: “In this study, NLR values were higher in the PPROM group than in the control group.” That finding supports further evaluation of hematologic ratios as pragmatic, system‑ready markers-provided they are validated, carefully governed, and embedded within guideline‑based care rather than positioned as a shortcut around established clinical assessment.