Retrospective HELLP case series underscores maternal risks and system demands
A newly published retrospective case series on hemolysis, elevated liver enzymes, and low platelet count (HELLP) syndrome adds to a growing body of evidence that this hypertensive pregnancy complication carries a concentrated burden of maternal morbidity and resource use. The report synthesizes clinical presentations and in-hospital complications from patients meeting HELLP criteria, highlighting that outcomes turn not only on disease severity but on how quickly hospitals mobilize multidisciplinary care, from obstetrics and anesthesia to intensive care and transfusion services.
While HELLP remains relatively uncommon compared with other hypertensive disorders of pregnancy, its complication profile is outsized. Evidence from population-level analyses in the United States shows patients with HELLP face the highest risk of cardiovascular severe maternal morbidity at delivery among hypertensive subtypes, elevating the stakes for rapid recognition, escalation pathways, and critical-care access within maternity services. These risks sit squarely within the broader effort to reduce preventable maternal deaths and severe morbidity being tracked through national quality initiatives and federal reporting requirements related to maternal health. cardiovascular severe maternal morbidity at delivery
What the researchers examined
- Study design: retrospective case series using hospital charts of pregnancies complicated by HELLP syndrome, providing granular clinical detail that is often obscured in administrative datasets.
- Case identification: laboratory-based diagnostic criteria consistent with established HELLP classifications (hemolysis, transaminase elevation, and thrombocytopenia), allowing comparison with existing clinical guidelines.
- Primary focus: frequency and type of maternal complications during antepartum or postpartum hospitalization; need for higher-acuity care and blood products; timing relative to delivery and to the onset or recognition of HELLP.
- Secondary observations: concomitant hypertensive features, gestational age at presentation, and perinatal context (e.g., preterm delivery, fetal status) as they relate to maternal course and decisions about timing of delivery.
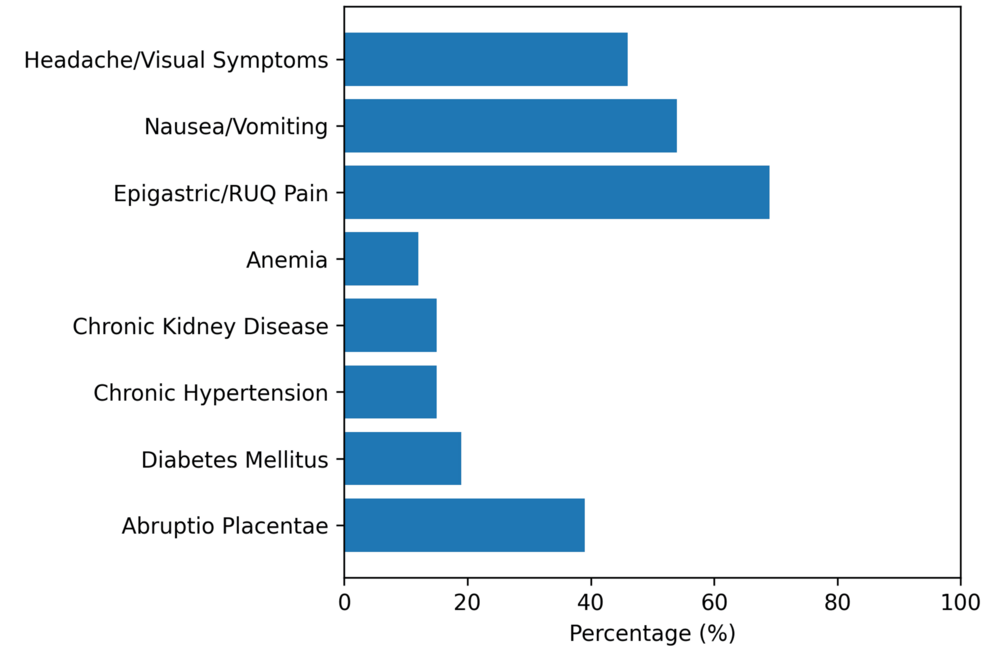
Maternal complications recurrently documented in HELLP
Across clinical literature and in this series, HELLP is linked with multi-organ complications that can develop rapidly before or after birth, often within hours of symptom onset:
- Coagulopathy and bleeding complications (e.g., disseminated intravascular coagulation, postpartum hemorrhage; frequent need for transfusion support).
- Placental abruption and related hemodynamic instability, sometimes preceding an emergency delivery.
- Acute kidney injury requiring close monitoring and, in severe cases, renal support or intensive-care management.
- Pulmonary edema and respiratory compromise; risk of intensive-care admission and advanced respiratory support.
- Hepatic complications ranging from subcapsular hematoma to rare rupture, with potential need for interventional radiology or surgical intervention.
- Neurologic events in the setting of severe hypertension or microangiopathy, including seizures and stroke.
Consensus clinical references describe HELLP as a life‑threatening entity with both maternal and fetal consequences, reinforcing the need for standardized emergency response inside maternity units and for hospital leaders to ensure those protocols are resourced and regularly rehearsed. consensus clinical references
When HELLP strikes: critical time windows
For clinicians, much of the risk in HELLP lies in its timing and sometimes subtle early signs:
- Typical onset: late second to third trimester in association with preeclampsia features, when patients are already under closer surveillance but may move between outpatient and inpatient settings.
- Postpartum vulnerability: a notable share of cases are first recognized in the 48–72 hours after delivery, demanding vigilant postnatal monitoring even after an apparently uncomplicated birth and discharge planning that accounts for delayed presentations.
- Atypical presentations: can occur with minimal or absent hypertension; symptoms may center on right upper quadrant pain, malaise, headache, or nausea, increasing the risk that HELLP will be misattributed to more benign postpartum complaints.
System and policy implications for hospitals and health authorities
Because HELLP compresses high-risk events into a short timeframe, it functions as a stress test of how maternity units, hospital systems, and regulators organize emergency obstetric care. In the United States, elements of this response are increasingly incorporated into maternal safety bundles and into facility-level expectations set by agencies operating under the Affordable Care Act, which expanded quality reporting and value-based purchasing in hospital care.
| Priority area | Operational implication in HELLP |
|---|---|
| Rapid diagnostic capacity | Round‑the‑clock labs capable of fast-turn platelet counts, liver enzymes, and hemolysis markers, with protocols for repeat testing as status evolves and for flagging critical results directly to obstetric and critical-care teams. |
| Escalation pathways | Clear triggers for maternal-fetal medicine, anesthesia, hematology, hepatology, nephrology, and ICU consultation; defined thresholds for transfer to higher-acuity settings, including regional referral when capabilities are limited. |
| Blood bank readiness | Immediate access to crossmatched blood, platelets, plasma, and massive transfusion protocols tailored for obstetrics, coordinated with pharmacy and laboratory services. |
| Hypertensive emergency response | Standardized order sets and drills for rapid control of severe-range blood pressures to reduce neurologic and cardiac events, aligned with national hypertension-in-pregnancy safety standards. |
| Imaging and surgical standby | Access to CT/ultrasound and interventional/surgical teams for suspected hepatic hematoma or abdominal catastrophe, with streamlined pathways from labor and delivery to operating rooms and radiology suites. |
| Postpartum monitoring | Structured surveillance after delivery, including nursing ratios that permit frequent vitals and symptom reassessment in the first 72 hours, and clear instructions for patients on when to seek urgent care after discharge. |
| Data and quality infrastructure | Real-time tracking of severe maternal morbidity, ICU admissions, and transfusions; participation in perinatal quality collaboratives and morbidity reviews, with HELLP cases flagged for system-level learning. |
| Equity and access | Mitigation of delays in recognition and transfer for patients facing geographic, insurance, or social barriers; culturally responsive communication and coordination with emergency medical services in regions with limited obstetric capacity. |
| Workforce training | Simulation and competency maintenance for HELLP and hypertensive crises across the obstetric care team, including nights/weekends coverage and contingency planning for staffing shortages. |
Key signals clinicians and health systems monitor
The case series underscores how a combination of laboratory trends, bedside symptoms, and resource utilization can alert teams to escalating risk:
- Laboratory trajectory: falling platelets; rising AST/ALT and LDH; evidence of hemolysis on smear or bilirubin trends, with attention to how quickly these values change over hours rather than days.
- Clinical red flags: right upper quadrant/epigastric pain, headache, visual changes, dyspnea, oliguria, altered mental status, or sudden hemodynamic shifts that prompt immediate reassessment and possible transfer to a higher-acuity unit.
- Resource‑use indicators: need for blood products, vasopressors, advanced respiratory support, or renal replacement—each a marker of acuity and potential quality‑of‑care gaps if initiation is delayed or if escalation requires out-of-hospital transfer.
Why this case series matters for public health
Although retrospective and limited to a specific institutional context, the findings echo broader concerns about maternal safety and capacity in obstetric care systems:
- Burden concentration: HELLP packages a high density of severe complications into a narrow time window, making system readiness—staffing, protocols, and interdepartmental coordination—decisive for outcomes.
- Measurable levers: standardized emergency protocols for hypertension and hemorrhage, faster lab turnarounds, and reliable access to critical care are modifiable at the facility level and can be incorporated into hospital performance measures.
- Accountability: incorporating HELLP-related metrics into maternal safety dashboards helps align hospital operations with state and national maternal health goals, informs regulators and payers assessing quality, and provides a concrete lens on whether reforms are reaching patients with the highest-risk complications.