Early-stage Alzheimer’s signal emerges as PPP2R5C falls in blood
A research team reporting in Cell Reports Medicine identifies a decline in the neuronal regulatory subunit PPP2R5C in blood that tracks with very early Alzheimer’s biology. The work positions PPP2R5C—part of the protein phosphatase 2A (PP2A) complex central to tau dephosphorylation—as a candidate plasma biomarker linked to the processes that precede cognitive symptoms.
Why this matters for health systems and policymakers: scalable blood tests are edging closer to routine triage for cognitive complaints in primary care and memory clinics. If validated, PPP2R5C could complement existing plasma markers (p‑tau181, p‑tau217, p‑tau231) and help health systems reduce dependence on costlier positron emission tomography (PET) and invasive cerebrospinal fluid (CSF) procedures for initial assessment, reshaping how limited specialist and imaging capacity is allocated.
What the study measured
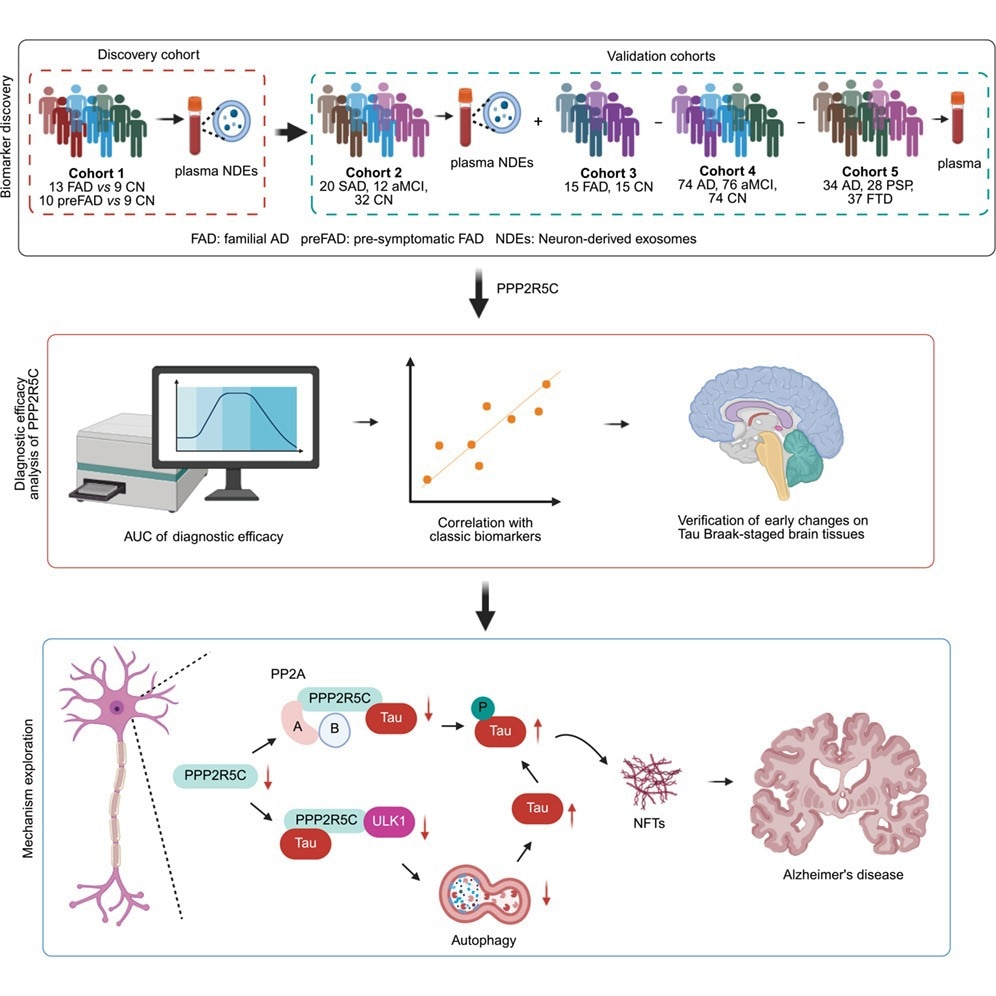
The investigation spanned neuron-derived exosomes (NDEs) and whole plasma across discovery, validation, and clinical cohorts, in both familial and sporadic Alzheimer’s disease. Key readouts are summarized below.
| Cohort/Matrix | Participants | Primary observation | Performance/readouts |
|---|---|---|---|
| Discovery (NDE proteomics) | CN (n=4); pre‑FAD (n=4); FAD (n=5) | PPP2R5C‑specific peptide progressively decreased from presymptomatic familial AD to symptomatic AD vs. cognitively normal. | Signal directionality established across the early disease course. |
| Validation (targeted NDE) | CN (n=32); sporadic AD (n=20); aMCI (n=12) | Reduced PPP2R5C associated with early AD‑linked processes. | Consistent pattern reproduced in sporadic disease. |
| Plasma (clinical comparison) | FAD (n=15); CN (n=15) | PPP2R5C significantly lower in AD than in cognitively normal controls. | Demonstrated that the NDE signal can be tracked in total plasma. |
| Plasma (aMCI/AD vs. CN) | CN; aMCI; AD | Group-level PPP2R5C differences vs. CN |
• aMCI: −61.3% |
| Discrimination (AUROC) | Plasma | Ability to separate clinical groups |
• AD vs. CN: 0.8494 |
- Correlations: Plasma PPP2R5C aligned positively with Mini-Mental State Examination (MMSE) scores and inversely with plasma p‑tau181, p‑tau217, and p‑tau231, reinforcing relevance to tau dysregulation and cognitive status.
- Neuropathology: Postmortem analyses showed lower brain PPP2R5C in AD versus both young and age‑matched controls. Immunohistochemistry indicated declines as early as Braak stage II, preceding extensive neurofibrillary tangle burden and supporting the notion that PPP2R5C loss is an upstream event.
Mechanistic signals mapping PPP2R5C to tau control
Together, mechanistic experiments connect the observed blood changes in PPP2R5C to intracellular pathways that regulate tau.
- Protein–protein interactions: Co‑immunoprecipitation demonstrated direct PPP2R5C–tau interaction, supporting a structural basis for PP2A‑mediated tau dephosphorylation.
- PP2A activation: Overexpressing PPP2R5C lowered phosphorylated and total tau while increasing PP2A activity; silencing PPP2R5C reduced PP2A activity, indicating that PPP2R5C levels modulate a core phosphatase axis implicated in Alzheimer’s pathology.
- Clearance pathway: PPP2R5C‑driven tau reduction was blocked by autophagy‑lysosome inhibitors (chloroquine, leupeptin, ammonium chloride) but not by the proteasome inhibitor MG132—implicating autophagolysosomal tau clearance as the dominant route.
- ULK1 axis: PPP2R5C expression negatively tracked with phosphorylated ULK1; docking and co‑immunoprecipitation supported a PPP2R5C–ULK1 interaction consistent with regulation of autophagy initiation. This provides a mechanistic bridge between PPP2R5C, PP2A activity, and tau turnover.
Where a PPP2R5C assay could sit in care pathways
For health systems facing rising demand for dementia assessment and constrained specialist capacity, a PPP2R5C assay—if confirmed in larger, real‑world cohorts—would sit within an evolving biomarker ecosystem rather than replace existing tools.
- Use case: As a minimally invasive blood marker, PPP2R5C could function as a pre‑screen alongside established plasma panels to prioritize patients for confirmatory PET or CSF testing, especially in primary care, community neurology, and telehealth triage models.
- Reference standards: PET and CSF will remain arbiters for biologic confirmation. Several CSF assays for amyloid and tau have been cleared for clinical use in the U.S., providing a regulatory and clinical reference framework against which any new plasma test would be judged.
- Analytical readiness: Transition from NDE‑based discovery to total plasma is promising, but laboratories will require harmonized pre‑analytical handling (collection tubes, processing times, freeze–thaw control) and cross‑platform calibration to keep between‑site variability low enough for clinical decision-making.
- Regulatory pathway: Most blood‑based Alzheimer’s assays currently reach patients as laboratory‑developed tests under the Clinical Laboratory Improvement Amendments (CLIA), overseen by the Centers for Medicare & Medicaid Services via the CLIA regulatory framework. A PPP2R5C assay intended for diagnosis at scale would likely require in‑vitro diagnostic clearance, with robust multicenter evidence, if sponsors seek broader distribution beyond a small number of reference laboratories.
- Coverage dynamics: Payer decisions increasingly hinge on analytical validity, clinical validity, and clinical utility. Evidence that PPP2R5C improves triage efficiency, shortens time to accurate diagnosis, or reduces downstream imaging and lumbar puncture demand would be decision‑relevant for public and private insurers.
Equity and system‑capacity considerations
The emergence of another blood‑based Alzheimer’s marker also raises distributional questions: who gets access first, and on what terms.
- Access points: Primary‑care‑orderable blood tests can broaden entry to cognitive evaluation where neurology capacity is constrained, particularly in rural and underserved urban settings where PET and specialist memory clinics are scarce.
- Population fit: The study emphasizes the need for larger, longitudinal, and ethnically diverse cohorts to ensure generalizability and to detect performance shifts across age, sex, and comorbidity profiles. Without this, PPP2R5C‑based decisions could entrench diagnostic inequities.
- Operational load: If adopted, laboratories would need validated reference ranges, quality‑control materials, and staff training to maintain low coefficients of variation at clinically relevant cutoffs, adding to workforce and capital planning for health systems.
- Ethical guardrails: Early biomarker positivity in people with minimal or no symptoms raises counseling and data‑privacy questions. Health systems should align communications, consent processes, and data governance with best practices for preclinical risk disclosure and genetic/familial counseling where relevant.
Key uncertainties and validation priorities
For now, PPP2R5C remains an experimental marker with clear promise but significant evidence gaps that regulators, payers, and clinical guideline writers will expect sponsors to address.
- Stage discrimination: The AUROC of 0.5931 for aMCI vs. AD indicates limited staging utility; clinical value may center on early‑stage detection (identifying individuals on an Alzheimer’s trajectory) rather than fine‑grained classification within the dementia spectrum.
- Comparators: Head‑to‑head performance against p‑tau‑based blood panels and in combination models (multi‑analyte scores that integrate amyloid, tau, and neurodegeneration markers) remains to be established.
- Confounders: Systemic inflammation, renal function, concurrent neurodegenerative conditions, and commonly prescribed medications should be evaluated for analytical and clinical interference, including false‑positive and false‑negative patterns.
- Neuropathological alignment: Prospective studies linking plasma PPP2R5C trajectories to longitudinal tau PET, CSF markers, and conversion from aMCI to AD will be critical to demonstrate clinical utility and to support health‑economic modeling.
- Assay standardization: Shared calibrators, reference intervals, and external proficiency testing are prerequisites for broad deployment and for inclusion in clinical guidelines and reimbursement policies.
What to monitor as evidence matures
Over the next several years, PPP2R5C’s trajectory will depend less on its initial biological plausibility and more on how it performs under real‑world and regulatory scrutiny.
- Multicenter, diverse cohorts with pre‑specified endpoints and blinded analyses, designed to satisfy regulatory and guideline expectations.
- Reproducibility across platforms and laboratories, including lot‑to‑lot stability and inter‑run precision, to support consistent use across regions and health systems.
- Integration into multi‑marker algorithms that combine PPP2R5C with p‑tau and neurodegeneration measures, potentially enhancing risk stratification for disease‑modifying therapies.
- Regulatory and reimbursement milestones that define where PPP2R5C fits alongside existing biomarker pathways and emerging Alzheimer’s treatments—from early coverage policies to its appearance (or absence) in formal clinical practice guidelines.
For readers seeking foundational explanations of biomarker science in neurodegeneration, see this overview of biomarkers from the National Institute on Aging.