The conceptualization of the human brain is undergoing a fundamental shift as researchers identify the mechanisms the organ uses to maintain its internal environment. Central to this evolution is the discovery of a waste disposal network-the glymphatic system-which may hold the key to understanding a range of neurodegenerative and systemic conditions.
For decades, patients suffering from myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) have faced systemic medical skepticism. The condition, characterized by profound exhaustion and cognitive impairment, was frequently dismissed as psychosomatic due to a lack of visible pathology on standard clinical tests. This lack of biological evidence often translated into a failure of healthcare systems to provide adequate support or recognized disability frameworks for millions of affected individuals.
The Mechanics of Neural Waste Clearance
The glymphatic system operates as a hydraulic cleaning mechanism, primarily active during sleep. This process is essential for preventing the accumulation of metabolic byproducts that can lead to neuroinflammation and cellular dysfunction. First described in detail just over a decade ago, it represents a distinct macroscopic clearance pathway running in parallel to the classic blood-brain barrier and immune system, rather than replacing them.1
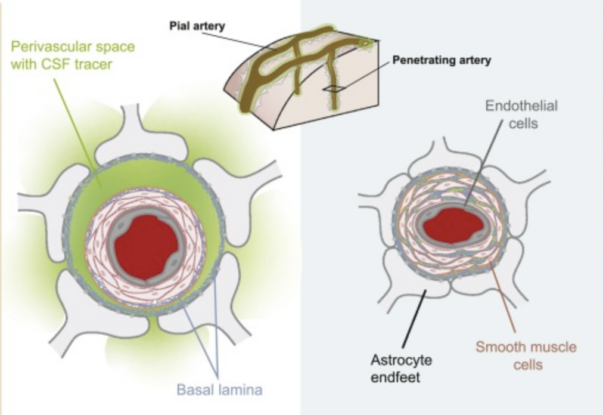
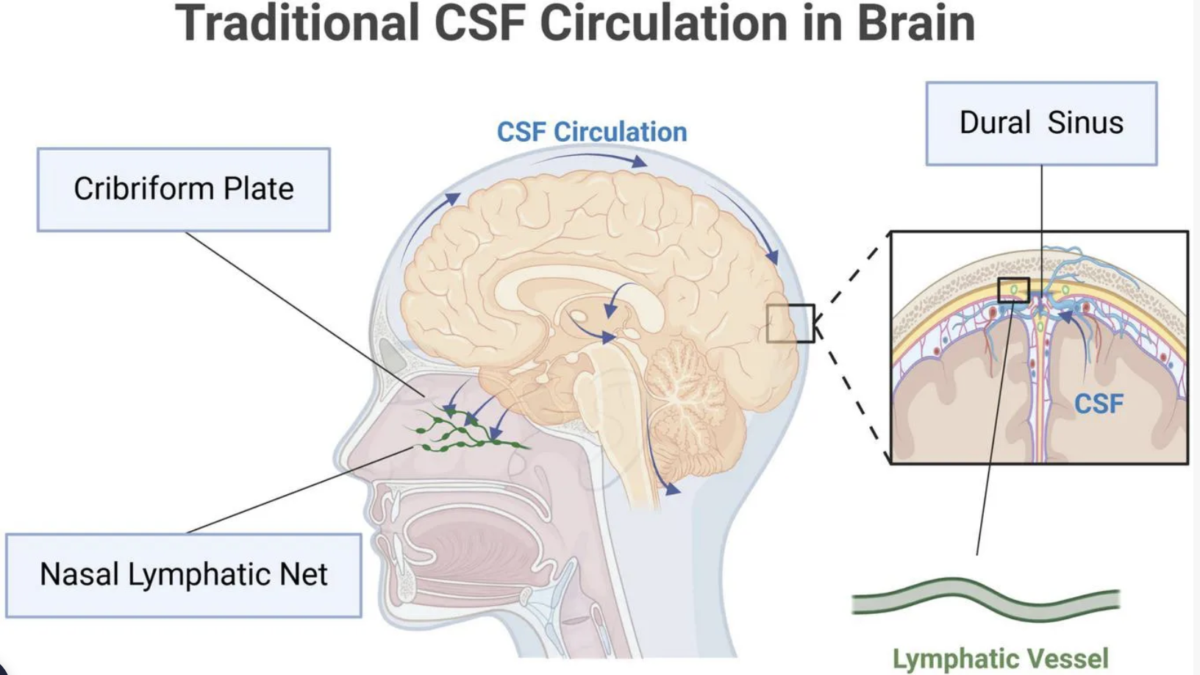
- Fluid Dynamics: Cerebrospinal fluid (CSF) is pumped through a network of perivascular channels lined by astroglial cells, flushing out dead cells, toxic proteins such as beta-amyloid, and other soluble waste products from the brain’s interstitial space.1
- Sleep Dependency: Clearance is most efficient during deep, slow-wave sleep, when these channels widen and CSF inflow increases, highlighting the physiological necessity of high‑quality sleep for long-term cognitive maintenance.
- Pathological Accumulation: Failure or slowing of this system can lead to the buildup of metabolic waste, which is increasingly linked to neuroinflammation, cognitive decline, and elevated risk in disorders such as Alzheimer’s and Parkinson’s disease.2,3
Biological Markers and the Shift in Diagnostic Paradigms
The movement toward biological validation for ME/CFS represents a critical turning point in public health. Identifying tangible markers allows the medical community to shift from symptomatic management to mechanistic understanding, potentially altering how the condition is coded, insured, and treated within national health infrastructures.
This shift is beginning to intersect with formal classifications. ME/CFS is already recognized as a neurological disease under the World Health Organization’s International Classification of Diseases, a framework that guides how conditions are reported, reimbursed, and monitored by governments and insurers worldwide via the ICD system. As imaging and molecular markers mature, they are likely to influence how severity is graded, how work capacity is assessed, and how eligibility for disability benefits is determined.
| Marker Category | Evidence/Findings |
|---|---|
| Genetic | Identification of eight specific genetic signals associated with immune regulation and cellular stress responses. |
| Systemic | Biomarkers found in blood, spinal fluid, and the gut microbiome that suggest altered energy metabolism and disrupted homeostasis. |
| Immunological | Links to systemic inflammation and immune dysfunction, including abnormal cytokine profiles and impaired antiviral responses. |
| Neurological | Impaired glymphatic waste clearance evidenced via MRI, correlating with cognitive and sleep-related symptoms. |
Hemispheric Asymmetry in Glymphatic Dysfunction
Recent research from Griffith University has utilized non-invasive MRI techniques to estimate glymphatic function by measuring the diffusion rate of CSF into channels surrounding small blood vessels. This approach avoids the risks associated with invasive tracer injections into the spinal canal and, crucially, makes the method far more compatible with routine hospital workflows.
The findings reveal that patients with ME/CFS exhibit reduced glymphatic function, specifically concentrated in the right hemisphere of the brain. This asymmetry is a significant detail, as similar patterns of disrupted perivascular clearance have been observed in patients with amyotrophic lateral sclerosis (ALS) and Parkinson’s disease, hinting at shared mechanisms of neuronal vulnerability across different conditions.
“This study is the first to demonstrate impaired glymphatic function in ME/CFS using MRI, providing a mechanistic explanation for the inflammatory changes reported by other Australian and international teams,” says neuroimmunologist Kiran Thapaliya. “This suggests that dysfunction in the brain’s natural cleaning system may be a key driver of this condition.”
The study noted a direct correlation between the degree of right-hemisphere dysfunction and the severity of “brain fog” and sleep disturbances experienced by patients. This suggests that the inability to clear toxic products may exacerbate central nervous system inflammation, directly contributing to neurological symptoms and possibly amplifying day‑to‑day fluctuations in cognitive capacity reported by many people with ME/CFS.
Implications for Public Health and Diagnostic Access
The ability to detect these changes via non-invasive imaging could fundamentally alter the clinical pathway for millions. Historically, the diagnosis of complex neurological syndromes has relied on the exclusion of other diseases, leaving patients in a diagnostic limbo that delays treatment and social support and often undermines their credibility in the eyes of employers and social insurance systems.
In countries where access to disability benefits and workplace accommodations depends on objective evidence, reproducible imaging markers of glymphatic dysfunction could reshape how occupational health services, insurers, and social security agencies assess ME/CFS. Clearer diagnostic criteria anchored in observable brain changes would also support more consistent application of existing equality and disability legislation, rather than leaving decisions to fragmented case‑by‑case judgments.
Sonya Marshall-Gradisnik, director of the National Center for Neuroimmunology and Emerging Diseases at Griffith, explains that these brain scans reinforce “the notion that sleep plays a critical role in maintaining brain health.”
“We hope the results can pave the way for better diagnosis through the use of non-invasive procedures, and importantly, future treatment for patients,” she adds.
From a policy perspective, the integration of such imaging techniques into standard care would require significant investment in neuroimaging infrastructure and specialized training for radiologists. Health ministries and payers would need to decide whether to reimburse advanced MRI protocols for ME/CFS assessment, and how to prioritize them alongside competing demands in neurology and oncology.
Yet the potential reduction in long-term disability costs and the improvement in patient quality of life provide a strong economic argument for the adoption of these diagnostic tools. For governments already grappling with the wider burden of post-viral syndromes following the COVID-19 pandemic, establishing evidence-based pathways for ME/CFS diagnosis and support could become a test of how quickly health systems can adapt to emerging science.
As neuroscience continues to map the brain’s waste clearance system, the focus now moves toward whether these pathways can be therapeutically targeted to restore neural health-through sleep-focused interventions, pharmacological modulation of CSF flow, or future devices that influence perivascular dynamics. For policymakers, the science is no longer an abstract curiosity about “brain plumbing”, but a developing field that could redefine how chronic, often invisible illness is recognized and resourced in law, in clinics, and in the workplace.